Breathing is the most ordinary of human acts, so continuous that it dissolves into the background of consciousness. Yet in clinical medicine it is one of the most scrutinised, and paradoxically, one of the most difficult to measure with precision, continuity, and nuance.
The recent convergence of radio-frequency engineering and clinical rehabilitation research, exemplified by work at Chalmers University of Technology, Sahlgrenska University Hospital, and the University of Gothenburg, suggests a subtle shift: the possibility that breathing may soon be monitored invisibly, continuously, and locally, using the same wireless technologies that track goods through global supply chains.
This development, centred on passive RFID tags functioning as sensor proxies, is neither merely technical nor merely clinical. It represents a rethinking of how bodily signals can be captured, interpreted, and integrated into healthcare systems.
The Problem of Measuring Breath
Traditional respiratory assessment is constrained by its own sophistication. Imaging techniques such as computed tomography and X-ray provide detailed anatomical insight, yet are expensive, hospital-bound, and expose patients to ionising radiation. Meanwhile, spirometry, the clinical mainstay, requires active cooperation and offers only global measures such as airflow and lung capacity.
There is, as the research team emphasises, a gap between precision and accessibility. Clinicians require detailed information about how different regions of the chest wall move during respiration, yet existing wearable technologies such as plethysmography belts or piezoelectric sensors lack spatial resolution.
This absence is not trivial. Many respiratory disorders manifest asymmetrically, affecting different lung regions unevenly. Rehabilitation, particularly after surgery or in chronic conditions such as COPD, increasingly demands personalised, localised analysis rather than global averages.
The challenge is thus conceptual as much as technical: how to measure a distributed, dynamic physical phenomenon across the body in a way that is both granular and unobtrusive.
RFID as a Medical Sensing System
Radio-frequency identification technology was not designed for this task. Its origins lie in logistics, retail, and tracking systems, where passive tags respond to reader signals and return identification data.
The conceptual leap in the Chalmers-led research lies in recognising that RFID signals do more than encode identity. They also encode motion.
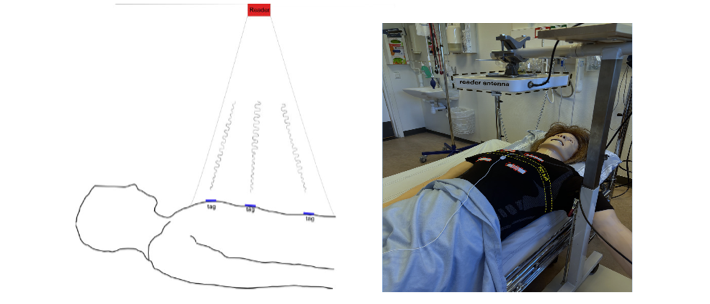
When a passive RFID tag is placed on the chest, its distance from a reader changes with each breath. These minute displacements alter the phase of the backscattered radio signal. By analysing this phase variation, it becomes possible to reconstruct breathing patterns and even quantify local chest wall displacement.
In experimental conditions, multiple tags are placed across anatomically meaningful points on the thorax. Each tag, uniquely identifiable, acts as an independent measurement node.
The implications are striking. Unlike radar-based systems, which struggle to distinguish signals from overlapping body regions, RFID inherently supports multi-point sensing because each tag transmits a distinct identity.
The result is a distributed sensing network on the patient’s body, without wires, without batteries, and without direct contact beyond a thin adhesive layer.
From Simulation to Signal
The research remains, at present, a proof of concept. Experiments were conducted using a programmable medical mannequin capable of simulating breathing patterns, including asymmetry.
Two configurations were tested: a two-tag system for bilateral comparison, and a four-tag system for more detailed spatial mapping.
The results are cautiously promising. RFID-derived measurements showed strong correlation with a reference piezoelectric respiration belt, with correlation coefficients often exceeding 0.70 and, in frequency analysis, 0.90.
More importantly, the system could detect asymmetry. When one side of the simulated respiratory system was deactivated, the corresponding reduction in chest displacement was clearly observed in the RFID data.
From a clinical perspective, this is perhaps the most significant finding. It suggests that the system does not merely measure breathing in aggregate but can distinguish local dysfunction, a prerequisite for targeted diagnosis and rehabilitation.
A New Clinical Imagination
The Swedish research and related reporting make clear that the ambition extends beyond technical feasibility. The goal is a transformation in how respiratory care is delivered.
Small, plaster-like tags could enable continuous, contactless monitoring in both hospital and home environments. Patients recovering from lung surgery or managing chronic diseases could be followed over time, with clinicians detecting deterioration earlier and intervening more precisely.
This aligns with a broader shift towards personalised and evidence-based rehabilitation. Rather than episodic measurement during hospital visits, respiratory function could be monitored as a dynamic, lived process.
There is also a profound infrastructural implication. Because RFID technology is relatively low-cost, widely standardised, and already embedded in many industries, its adaptation to healthcare could lower barriers to advanced monitoring.
In this sense, the innovation is not only the sensor but the ecosystem into which it fits.
Limits, Noise, and the Physics of Reality
Yet the research paper itself remains clear-eyed about limitations, and these are neither minor nor easily resolved.
The most persistent challenge is multipath interference, a phenomenon in which radio waves reflect off surrounding surfaces and interfere with one another. This can distort measurements and undermine stability.
In controlled environments, careful positioning of the reader mitigates the issue. In real-world settings, full of reflective surfaces, moving bodies, and electromagnetic noise, the problem becomes significantly harder. Another limitation concerns the hardware itself. Commercial RFID systems are not designed for high-resolution motion sensing. They impose constraints on data access, signal fidelity, and configuration.
There are also biological complexities. Human bodies are not mannequins. Movement, posture changes, and soft tissue dynamics introduce variability that may degrade signal quality. Even the seemingly trivial issue of keeping a tag properly attached to the skin can affect measurement reliability.
Finally, there are questions of electromagnetic safety and compatibility with medical devices, particularly implanted ones. These constraints underscore a broader point. The translation of a sensing technique into clinical practice is not simply a matter of accuracy but of robustness, safety, usability, and integration.
Between Engineering and Care
The deeper significance of this work lies in its interdisciplinary character. It is neither purely biomedical nor purely technological. It requires collaboration between electrical engineers, physiotherapists, clinicians, and data analysts. The presence of institutions such as Sahlgrenska University Hospital in the research reflects this necessity. The questions being asked are not only “Can we measure this?” but also “What does this measurement mean for patient care?”.
This dual orientation is evident in the emphasis on rehabilitation. Breathing is not simply a diagnostic signal; it is a behaviour that can be trained, modified, and restored.
If RFID-based sensing can provide detailed feedback on regional breathing patterns, it may support new forms of physiotherapy, where patients learn to engage specific parts of the thorax more effectively.
Towards an Invisible Medicine
Perhaps the most intriguing aspect of RFID-based breathing monitoring is its invisibility. The system operates at a distance, without requiring active participation or even awareness.
This raises questions that extend beyond the technical domain. What does it mean for medicine when monitoring becomes ambient rather than episodic? When the body is continuously translated into data streams, interpreted in real time, and potentially acted upon automatically?
RFID technology, in its original context, was about tracking objects. In this emerging medical context, it becomes a means of tracking processes, subtle, rhythmic, and inherently human.
The breath, once measured in forced exhalations and clinical snapshots, may instead be observed as a continuous signal, unfolding over hours, days, and weeks.
The transition is quiet, almost imperceptible. A thin adhesive patch on the chest. A reader emitting radio waves. Data flowing silently into analytical systems.
Yet within that quiet change is a significant reorientation of healthcare, from intermittent observation to continuous presence.
The research on RFID-based breathing measurement does not yet represent a finished technology. It is a careful, incremental demonstration of possibility.
It shows that with relatively simple components, it is possible to capture complex physiological behaviour in a distributed, non-invasive, and potentially scalable way. It also shows that translating this possibility into practice will require addressing substantial technical and clinical challenges.
What emerges most clearly is not a single innovation but a trajectory. A movement towards measurement systems that are local yet global, precise yet unobtrusive, and technical yet deeply embedded in the human experience of illness and recovery.
Breathing, once the simplest of signs, may become one of the most richly understood.
References
- Zeng, X., Wu, J., Thelandersson, A., Kjellby Wendt, G., & Fagevik Olsén, M. (2026). Localized measurement of breathing movement using RFID: Proof-of-concept and challenges. IEEE Access, 14, 12655–12663.
- Sahlgrenska University Hospital. (2026, April 15). Ny forskning: Etiketter som mäter andning ska hjälpa lungsjuka. [sahlgrenskaliv.se]
- SVT Nyheter. (2026, April 15). Chalmers och Sahlgrenska testar etiketter som mäter andning – ska hjälpa lungsjuka. [svt.se]